I’d be willing to bet that you generally don’t like to be in pain. I’d be willing to bet more that you really don’t like it when kids and teens are in pain. Chances are, if you are the parent of a young athlete, your child or teen has been in pain at some point in their sports “career.” Maybe you knew what to do about it and your child got better without any problems. Maybe you had no clue and turned to your friends, Dr. Google, or relied on your own steadfast remedy system.
I’ve encountered a gazillion parents who fall all over the map of knowing how best to care for their children’s pain. Sometimes parents make decisions about how to care for a child’s pain that ultimately leads to worsening of the problem. These decisions may be based on an interest to keep a child playing a sport for a number of reasons. On the other hand, some parents fall more into the “hypervigilant” category. These are the parents who fast track their children to the urgent care center every time Johnny or Sarah complains of an ache or pain.
Despite a parent’s style in caring for pain, one thing all of these parents have in common is that they mean well, regardless of which way they handle each situation. Culture and experience lead people to act in different ways, but there are a few constants that hold true in caring for a child or teen’s pain regardless of one’s background.
Given that I happen to work with young athletes of all ages, I often get questions from patients, colleagues, friends, and family members about pain in their own or their friends’ children. Here is a sampling of the questions I am asked quite frequently:
“My 12 year old has been having ankle pain off and on for 3 weeks. She’s been wearing a brace and keeps doing her sport but she says it’s getting worse. When should I panic and do something about it?”
“My 8 year old just fell off the monkey bars, says his elbow hurts, and refuses to move his arm. I have 3 meetings I need to attend and he has a baseball game tonight. Can we wait and see how it feels tomorrow?”
“My 15 year old’s back has been hurting for 6 months and it’s getting worse. She has bad posture. I told her to stretch and do some yoga with me since that’s what helped me. We also put her on our home traction table, I let her use my TENS unit, and she’s been getting chiropractic adjustments from my chiropractor 3 times per week.”
“My friend’s 13 year old has mysterious abdominal pain and has been out of school for 6 months. Nobody can figure out what is wrong with her. Is there another specialist she should see or is this all in her head?”
“My 17 year old has hip and groin pain. I think it’s a hip flexor injury. She just needs to stretch her hip flexors and do some Pilates, right? Can you show me some stretches for her to do?”
<Spoiler alert: If any of these situations sound familiar, you’re not alone! We will revisit each of these situations—and what to do about them– in a future blog. Stay tuned!>
Parents, friends, coaches, and kids and teens themselves have lots of questions about how to deal with pain. This can be very confusing, and everyone has an opinion on it. Before we address the somewhat confusing question of how to deal with it or what to do about it, we must first address the possibly more confusing topics of what pain is and what this could mean in a kid or teen.
Defining Pain
The first thing we need to do is define pain. Get ready for a blast back through science class. A person can perceive and experience pain for any number of reasons. According to the International Association for the Study of Pain, Pain is “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.” What that means is there is not always damage somewhere in the body when pain is present. If that’s the first time you’ve heard that, you’re not alone. What we know about pain barely scratches the surface of what lies beneath the understanding of why it occurs.
Pain is an output from the brain
One thing we do know is that pain is absolutely, positively, 100 percent produced as an output from your brain. See this great youtube video to explain this. While the video is about chronic pain, the same concept applies to just about any type of pain.
Think of the body like an email communication system. You bump your knee, and your ultra-fast email system sends a message through your nervous system to a part of your brain that acts as a switchboard. The switchboard decides if the message is relevant and if it merits being sent on to any other part of the brain. What you need to know about the switchboard is it is not in the conscious part of your brain. If the switchboard deems the message relevant, it sends the message along to your cerebral cortex. This is the part of your brain where you make thoughts, perceptions, and do all the cool, complex processing that makes us human. It’s not until the email message gets to your cortex that your body then decides “oh wow! Bumping my knee hurts!” Thus, it is an output, or a decision, just like any other decision you make.
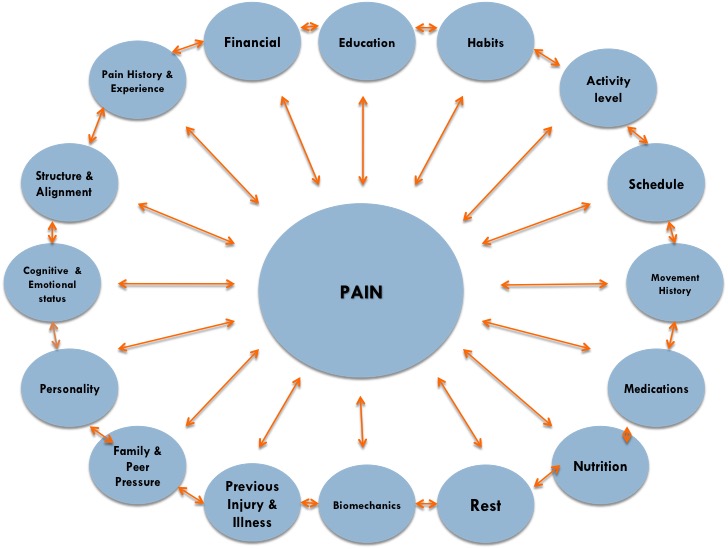
Now you may be thinking here “Ok Julie, I didn’t decide that I wanted to be in pain.” That’s right. You didn’t. But your conscious brain did. Due to wiring in your brain that you’ve been formulating since before birth-your brain decided whether or not that knee bump was going to be painful. The combination of your life history, culture, environment, previous experience, previous pain and injury, overall health status, emotional status, and many more factors – things that you sense and direct every day—was responsible for deciding if that bumped knee was going to hurt or, well, just feel like you bumped your knee.
You can think of pain in a kid like a wheel–it’s totally dependent on so many factors. These factors include intrinsic ones (stuff within the kid that can’t change, regardless of what is going on around the kid), and extrinsic factors (stuff that can change–IE the environmental factors going on around the kid).
Notice that I said perception of pain is based on factors like life experience, previous pain and injury, and emotional status. Those are just a few factors that might make pain perception a little different in kids. Why is that? Kids have less life experience, likely fewer pains and injuries, and emotional and cognitive/thinking statuses that are not fully developed. This makes pain perception very different for them.
If things are going well, most kids experience the occasional bump, bruise, scrape, splinter, or “owie” as my 21-month-old niece likes to call it. Most “kid pain” gets better with a kiss from mom and dad, maybe a band-aid, and encouragement to “shake it off.” Healthy kids without serious problems are often seen to be running, jumping, and playing through pain. It’s not until pain slows them down or changes their behavior that it usually registers on parents’ or coaches’ radars.
What this means is that as kids develop, they may not know exactly what is going on with their pain. They often don’t have the experience or previous pain and injury to be able to describe it. This can make it hard for parents, coaches, and healthcare providers to understand how to help them.
Oftentimes kids learn how to describe pain based on what an adult tells them it should feel like. Case in point: I’ve had an 11-year-old tell me that her knee feels like “bone on bone.” In actuality, this is how physicians or patients may describe an extremely arthritic joint in someone who is a middle-aged adult and has lost all cartilage cushioning in the joint. While not impossible, it’s not something that we would typically expect a ‘tween to say. Ask a 7 year old to describe the pain and they will give you a blank stare. They just don’t have the experience, the complex thinking processes, or the knowledge to know how to describe it. Typically they will just agree with whatever an adult says.
Not only do we have the challenge of getting kids to describe what’s going on, but kids’ behavior around pain is also all over the map. Depending on influence from adults, siblings, and friends who may have pain or have loved ones in pain, kids learn how to behave and perceive pain from those around them. Some kids learn from a very young age that pain is scary. They may panic or complain constantly about every ache and pain. They may also learn that being in pain is a way to get support, attention, or avoid an unwanted activity. This would mean the real underlying problem may not actually be related to the pain at all (more on that later).
Other kids may learn that “being tough” while in pain is admirable and brave. These kids may not complain at all when they probably should be. This means you may have one kid who has a total meltdown over a splinter, and another kid who seems calm and collected over a broken leg. As you may imagine, there’s clearly a fine line to walk here in teaching kids and teens how to cope with pain. We don’t want to panic them, and we don’t want them to be heroic at the expense of hurting themselves more. And even if you think you’re toeing that line just right as a parent or coach, chances are they’re learning about pain coping (and everything else kids, ‘tweens and teens learn) from other outside influences, too.
Needless to say—pain is complex in any person, regardless of age. Add a developing brain, body, and lots of family and sports influence in the young athlete—and we have the potential of launching those complexities to exponential levels.
Now that you’re armed with more knowledge than you ever wanted to have about what pain is and what it means in a child, teen, or young adult, you’re probably asking–So what do we do about it?
Stay tuned for Part 2 to learn how to address and cope with a child, ‘tween’s, teen’s, or young adult’s pain situation.
What if I told you that there is a muscle in your body that is key to giving you good posture and participates in weight lifting between 17,000 and 25,000 times per day? What if I told you it does this without you even knowing it? What muscle do you think that is? Hint: it’s not a heart muscle.
Stumped yet? Check out this great blog by my colleague Jessica Reale to find out the answer. Young athletes of all ages and backgrounds need to learn from a young age the importance of this muscle.
I have a small confession to make– I love the study of human anatomy. Always have. It was studying human anatomy and physiology that made me shift my undergraduate degree at Gordon College away from “Biology” and into “Movement Science” (which has now become “Kinesiology”… Who would have known that years later, “Movement Science” would have been the coolest name for a major ever? Am I right fellow PTs?). The human body is fascinating and incredible. So, it should come as no shock to you that I have favorite muscles. In PT school, my favorite muscles were the ones with the most fun names… like the Gemelli brothers (who are small hip external rotators) or Sartorius (a thigh muscle…best, if sung to the tune of “Notorious“). Of course, you know that now the pelvic floor muscle group ranks pretty high on that list…but the diaphragm, well… it just takes…
Female athletes have a million awesome attributes that make us way cooler than boys. Girls rule and boys drool, right?
Even though we are sugarier (word invention), spicier, and everything nicer than our male counterparts, we have some unique considerations to worry over that sometimes make being a female athlete a challenge.
Maybe you were a female athlete from a young age. Think back to your first competition, meet, match, or game. For me, it was at age 6 in a summer league swim meet. I fell in love with the sport and the rest was history.
Dedicated to my sport, I raced through the rankings and ended up training 8-9 practices per week by 8th grade. Little did I know that the 2 fractures I had as a teenager were warning signs of a potentially bigger problem. Yikes. And little did I know that the “mental slump” I was in during high school and the depression that set in when I could not swim after shoulder surgery in college might catch up to me later.
How annoying is it that I can look back and see so many of these warning signs for things that became bigger issues later? How much more annoying is it that there’s nothing I can do with my current knowledge and skills to go back and help young athlete Julie? I guess that’s why I dedicate my career to doing that for everyone else.
If only it were that easy.
Parents and athletes often resist or fight against the education I so eagerly want to provide them and—perhaps most notably—that they are paying me to give them. I regularly hear or encounter phrases like these. Maybe you’ve heard them too, or said them yourself:
“Oh, that couldn’t possibly apply to my daughter”
“Injuries and burnout are ‘normal’ and expected for this particular sport”
“Of course she loves the sport! Look at how well she is doing!”
“She couldn’t possibly take time off or give up the sport. It’s the only thing we have getting her into college!”
I had a meeting with an awesome pediatric/adolescent sports medicine physician this morning and we commiserated over these phrases we so often hear, in addition to several other topics that young female athletes and parents just don’t love to discuss or address—but so desperately need to.
Yeah ok, I get it. Your daughter is flawless and invincible. She is actually an exception to the rules, statistics, and science behind health and wellness in young female athletes. And this is because of her natural talent and passion and of all the money and time you put into allowing her to succeed, right?
I will never fault a parent or loved one for doing what they think is the right thing to do. Most or all of these phrases and thought processes are 100 percent uttered out of caring, good intention, and well meaning. But sometimes—just sometimes—it’s possible people just don’t know any better. That’s what those of us who have personally been there as the athlete, and who now work in this field, are here to help you understand.
Regardless of what you believe or support, what we can all agree upon is that no parent or athlete has a crystal ball. None of us in the medical and sports medicine world can predict the future, either. BUT-we do have a little bit more gypsy skill than meets the eye. We can look back and use our clinical judgment to determine what types of behaviors and movements might lead to a problem in the future. And great news!!! We’re actually on your side! We want to help you and your daughter succeed! So just read and listen for a few minutes. Here are some key points you should know about how you can help her too.
It’s not about you
This should go without saying, but unfortunately, I’m finding I still have to say it. This means it’s a real issue out there, folks. Susie’s gymnastics competition may, in fact, be a fashion competition for moms. You are convinced the only way for your 5 year old all star cheerleader will win a national championship is with her belly hanging out, 5 pounds of makeup and bling, and hair extensions. Maybe there’s an unwritten competition for which family provides the best, most organic, gluten free, Pinterest-worthy snacks after the baseball game. Or maybe you’re sure your 6th grader is going to be the next basketball star, just like you were in college. This means you have to be at every practice, on the edge of your seat, letting your blood pressure go through the roof and finding all the flaws in the referee calls because some other kid just outscored your kid. I get it. You mean well. And these are real things that actually happen. It’s likely that as parents, you get caught up in them. That’s fine. But do your daughter a favor: keep the attitudes and the behaviors to yourself. You may not realize it but she is watching you. Chances are, she is internalizing how YOU feel about her sport, and this could eventually backfire. Make her sport all about her.
Milk: it does a body good
Disclaimer: Dairy allergies and sensitivities are real. I respect that. This is not actually about milk, but I needed something catchy to get your attention. Did you know that almost all of a young female’s bone health is built and stored before she reaches her 20’s? Flash back to teen Julie and her stress fractures. Did you know that the biggest risk for a stress fracture is a prior history of fracture? Bummer for me and my 30-something bones now. That’s what my allergist meant when she told me that being on inhaled steroids as a teen with asthma and participating in non-weight bearing exercise could adversely affect my bones. How are you ensuring that your daughter is getting the right amount of calcium, and the essential vitamin D to help her body absorb the calcium and build strong bones? Maybe let her play outside in the sun a little—with adequate sun protection but not so much that she doesn’t get the natural healthy effects of sun exposure. And maybe let her have that fro yo she’s been begging you for.
Don’t be afraid to discuss menstruation. Period.
You wouldn’t believe how many people I freak out when I ask them about menstrual history. What’s the deal here people? You are female. You are over age 9 or 10. It’s part of your life, or soon to be part of it.So much a part of your life—that if it is NOT happening—we have some reasons to be majorly concerned. So let’s talk about it! While the age of menarche-the onset of menstruation-varies widely from girl to girl, it’s important as parents and medical providers to be having conversations about it BEFORE it’s time for her to begin menstruating. Why? Did you know that being an active female affects estrogen and progesterone levels and exercise in excess can lead to irregular menstrual cycles? Add on stress, rigors of school, and possibly inadequate nutrition: and those young girls’ periods are at risk of being jeopardized. Problems with hormone fluctuation are often seen by young girls in certain sports as “cool”–as in–you’re not cool unless you’re skipping periods. Why are they learning this and from whom did they learn it? Sure, not having to deal with the hassle each month sounds awfully appealing from time to time. However, knowing thelasting effects this phenomenon has on reproductive, bone, endocrine, mental, and physical health is important. We need to teach each girl that menstrual irregularity is just as concerning as discovering a bad zit on her chin the morning of school pictures.
She CAN be a Disney Princess: preferably Sleeping Beauty
Why are girls skipping periods? There are lots of reasons. One of them is too much energy spent for the amount of rest provided. This is called a RED-S, or relative energy deficiency in sport. You may have heard of this concept referred to as the Female Athlete Triad before. It’s all about energy. Energy is a math problem (sorry if you hate math). It is the sum of rest (physical, mental, and emotional) and nutrition minus the energy lost during exercise and daily life. See the equation:
Energy = (Rest (physical, mental, emotional) + Nutrition/Calorie Intake) – Caloric Expenditure (energy lost during exercise/daily activity/metabolic activity)
The body is smart. If energy is lacking, it will steal it from the energy used to do other things, notably that which is used to produce hormones and run the reproductive system. You may think “Susie is not going to reproduce for another 15-25 years, what’s the big deal? Hello! This is NO BUENO people! Lack of estrogen has a strong correlation to later infertility, poor bone health (read: osteoporosis), in addition to problems with the adrenals (stress hormone producers). She needs those stress hormones to build adrenaline, stay awake in school, take an exam, and participate in her sport! This can have a dramatic effect on her later in life. So for that young female who is practicing 40 hours per week, she needs to get just as much energy input through nutrition (see point below), but also through sleep. To add insult to injury—she probably isn’t sleeping as much for education and social reasons. Isn’t it every kid’s dream to stay up late? That’s a normal part of childhood/teen rebellion. Not to mention she may be up all night doing homework for her 37 AP classes and SAT/ACT/MCAT prep classes (MCAT? Isn’t that an exam for college students? Of course it is! But Susie will start studying at 14 for it!) If she truly loves her sport, she needs to learn that sleep will help her jump higher, run faster, and shoot better. And help her make her 4.5 GPA and ace the MCAT. Sleep hygiene is a habit to address when she is 6, not when she is 26 and running ragged in medical residency.
The drama llama: Kid problems are REAL problems
For the next paragraph, we’ll completely flip the situation and blame little Susie for all of her problems. This means you’re off the hook mom & dad, right? Wrong. Susie’s brain is NOT like yours, mine, or her older college age brother’s. This means that it is completely normal for her to be a dramatic, rollercoaster riding, irrational and emotional kid/teen. Why? Because she is a growing kid/ teen and we can’t stop that! The female brain processes and responds to information very differently than the male brain. In addition, she’s growing. Just because she is good at her sport and makes good grades, that does not mean her developing brain is equipped to handle the real problems of childhood, ‘tween-hood, and teenage life. You know what I’m talking about here: how that swimsuit looks on spring break, who she will dance with at the 7th grade dance, if she will try beer at the 9th grade birthday party (or if she will get invited), how many instagram “likes” and emoji tag-backs she got yesterday, and how to talk to YOU (her parents) about the fears and anxieties she faces as a young woman, including her opinion on how you parent her. Those are the real problems that often preoccupy her mind and affect her performance in her sport and her schoolwork. Plenty of scientific evidence supports the fact that a young female’s brain does not fully develop emotionally and cognitively (IE, the ability to feel, think and process) until her mid-20’s. She cannot process, communicate, and understand things the same way you and I do. And even then, some brains never develop those skills. Every girl needs a valuable mentor to help her navigate through all of her perceived life-or-death problems. Make sure she has that.
The apple does not fall far from the tree
Speaking of role models, it’s important to remember the old adage I wrote above. Girls learn how to act from their parents. If you’re a 2 times-a-day gym rat, she will think that is normal and the right thing to do. If you eat the whole box of Samoas while stressing over the girl drama you face at work, what do you think she will do when she is faced with drama among her peers? What happens if you are the overachieving parent who fills his or her plate with 300 (Well-meaning) activities with little down time? What do you think she will do with her spare time? Fill it! Some of the biggest predictors of problems in young girls are the problems faced by their parents. These could be medical, social, emotional, or financial problems. That is not anything to be afraid of. It’s important to be aware of your own vulnerabilities, acknowledge them and most importantly-model that you are taking a stand to take care of them yourself. If you take care of yourself, she will be taken care of too.
You are what you eat
I’ve already touched on this several times throughout this post. An athlete is only as good as the fuel she provides for her body. My colleague Mandy says “You wouldn’t try and drive across the country without putting gas in your tank and checking your oil, would you?” The same goes for the body. Most athletes and their families underestimate how many calories they burn throughout the day in addition to during a sport. This means they also underestimate just how many calories they need to be taking in. It’s all about energy availability for a healthy athlete. Consult a pediatrician and sports dietician for the best advice.
Variety is the spice of life
Believe it or not, Susie likely has interests outside of horseback riding. She may have her room decorated with posters of horses, ribbons, and ask for a horseshoe-shaped birthday cake. Problem is, she may not know what those interests actually are. Why? Let’s pretend she began to specialize in equestrian at age 8. She was so good at it that it’s all she wanted to do. You’re thinking “I just want her to be happy and do what she loves” and maybe “sweet! College scholarship in the making,” so naturally, you reinforce this behavior. Why wouldn’t or shouldn’t you, after all, that is good parenting. I agree. There is more to it, though. What happens when Susie gets hurt at age 13 and can’t ride for a few months? Maybe she has school to fall back on. But maybe not. Equestrian has been so rooted in her identity that she may begin to experience symptoms of anxiety and depression when she cannot participate. She has no idea who she is or how to define her successes and failures. Everything feels like a failure if it’s not equestrian. Compound that with the fact that she may have been so dedicated to her sport that she cannot identify several other interests to keep her busy, and you now have a snowball effect. As adults, we know that this does not make logical sense. However, to a teen-this can be world ending for them. We have to protect them and give them skills and mentoring to honor themselves and their passions-whatever those may be. Girls don’t have to be the all star at 50 different activities, but it’s important to have other activities on which to fall back. After all, remember that when she is an adult, she may not have the time or money to ride horses anymore. Make sure she has other things to keep her engaged and enthusiastic about life. It will pay off in the long run.
No pain no gain
Ah, finally. A moment to write about the “PT” part of this post. Playing through pain and injury is not, I repeat, is NOT admirable! With the exception of Kerri Strug in the 1996 Olympics, nobody is going to look back on their life as a young athlete and say “wow! I am so glad I played on that sprained ankle! Look at all the fame and admiration it brought me.” Pain in a young athlete is most often not anything majorly serious, but it is a sign that something is going awry in how they are moving, that they are not getting enough rest, or that their tissues are not able to heal. This means those same tissues will not help them perform as well. Their performance will suffer. Pain is not just “growing pains” that they will “grow out of.” A brace and some KT tape will not fix the problem. At a very minimum, get them checked by a pediatric/adolescent sports medicine physical therapist or physician and make sure you’re not ignoring an issue that could rear its ugly head months or years down the line. The small investment in time and money doing that for your young female athlete will make a world of difference in the repercussions it may cost her later.
Have a Plan B, C, and D
Lastly—college scholarships, professional sports, or whatever end game result you’re looking for may not ultimately happen. There are thousands of reasons that it could all work out, and thousands more that it may not. It’s important for every young athlete to have an adult facilitate for them a plan B, C, and/or D. It’s important to be active and healthy (the repercussions of not being active are far worse), but it’s important to balance that with being a kid, being healthy, and going about it the right way. Nobody is perfect. Even if you followed all of this advice (which, admittedly, is far from comprehensive), something still may go wrong. Be there for her when it does and help her unleash her plan B.
In summary:
You may have noticed a habit or behavior you’ve done at some point along the way–either to yourself or your young athlete. We’ve all done them! That’s ok! Nobody is perfect, and nobody has all of the answers. But now that you’re armed with some information and tools, you can start to pave the way to a healthy, successful, athletic life for your young female athlete. These things are arguably more important than any practice, costume, Pinterest snack, hair extensions, or $400 swimsuit you could possibly provide. That’s what we call “sponsoring” your athlete. Nike is a sponsor to sports teams and provides all of those things-but you better believe they don’t consider themselves parents of the same athletes. Girls need your awesome sponsorship, but also your awesome parenting skills. This means support, guidance, and unconditional love regardless of how well they perform or how much they truly love their sports. It’s our job as grown-ups to give that to them–and most importantly, ensure that the number one priority for all athletes is that they are having fun.
After watching my Duke Blue Devils conquer the ACC Women’s Swimming Championship at Georgia Tech this weekend, I spent the better part of my weekend devouring some great TED talks. Not only were the messages by Shirzad Chamine and Brene Brown inspiring and refreshing, but they also gave me the opportunity to reflect on my own recent public speaking experiences.
Two weeks ago, I had the honor and privilege to do what I consider two of the most humbling experiences of my professional life: speak with and in front of colleagues at the American Physical Therapy Association’s (APTA) Combined Sections Meeting. In keeping with the fact that it occurred the same week as the Super Bowl-we’ll basically equate this to the Super Bowl of all PT nerd-dom, complete with fanfare, its own hashtag, an exhibit hall with plenty of games and freebies, and plenty of evening parties. Just imagine 10-15,000 of your best nerdy PT friends all descending on one giant convention center in snowy, frigid Indianapolis (seriously, whose idea was that?). It was a geek fest- but a very inspiring geek fest at that. And some may argue it offered some great people watching and fashion critiques. Apparently the token wardrobe for PTs is still believed to be khakis and polos, if you were wondering (there is an entire Twitter conversation about that).
They even decorated the stairs with nerdy PT-isms
I found out last summer that I would be speaking, so there was plenty of time to prepare. Like the athlete that I am, I spent weeks training, rehearsing, polishing, and preparing my presentations so that I could get up there and deliver the presentations in true TED talk style. I read a book, watched tons of TED talks, and ran the talks by several colleagues and students. I selected outfits that would convey my personality. People: I wore HEELS for crying out loud. I spent hours in the convention center’s “practice room” making sure that the computer and projector were compatible and that all of my photos and videos shone through to convey my visual message. An audiovisual snafu was a worst nightmare for this overprepared, overachieving, nerdy PT.
Completely relaxed and confident, I walked into presentation 1, plugged in my computer for one final test, and it popped up beautifully onto the screen. I was speaking among 10 other experts in sports medicine. I was 7th in line to speak, covering a case study of a young female athlete swimmer (does it get anymore exciting for me!?). I sat listening to my colleagues share their stories, eagerly awaiting my turn to take the podium. It was finally my turn. I thought in my best Kevin McAlister homage “This is it, don’t get scared now,” proudly took the stage, and plugged in my computer.
Womp womp.
As Murphy’s Law would have it, all of those hours of preparation and practice came to a screeching halt. The A-V connection wasn’t working. What!? I’d practiced and tested it a minimum of 23495 times on this very projector! Why wasn’t it working? I had approximately 1 minute to get it sorted out before they told me to get off the stage and let the next speaker go. That 1 minute went pretty quickly and unsuccessfully, and off I went, sheepishly back into the audience.
Now, this could have been a total game changer. First time on a big stage and my computer malfunctions. The whole world can now seemingly assume that I wasn’t prepared. But…but..I practiced!! I swear! And I even bought the special Mac adapter! A charitable stranger offered up his PC computer and I spent 20 minutes transferring files, videos, and completely rewriting my talk. Apparently presentations written on a Mac don’t always transfer perfectly to a PC (Insert elitist Apple statement here). I finished everything just in the nick of time and retook the stage.
Talk 1: The Long Term Effects of Slipped Capital Femoral Epiphysis (SCFE) in Young Female Swimmer, part of the Sports Section’s Complicated Patient Session
By this time, I was going last. Nearly half the room had emptied as people left early to catch lunch. It wasn’t what I had envisioned. But I charged on. To my surprise, I was even more relaxed this time around. I thought, I suppose it can’t get any worse… The projector worked, I didn’t even need to consult my notes, and I delivered the message with ease and grace—even inserting a little humor here and there. After the talk, I had some wonderful conversations with PTs and PT students who were so thankful for a talk about swimmers-a topic that is rarely covered in a sports medicine world heavily focused on more traditional sports.
Thanks to the faithful who stuck around to see me dressed in a Missy Franklin costume!
First talk down. Snafus aside, I was pretty proud of myself. Now that I had ripped off the proverbial Band-aid, I was more than ready for the 2nd talk the next day.
For the next presentation, I was speaking with 2 of my most valued mentors and colleagues-Blair Green & Julie Wiebe. See this post and this post and this website to learn more about Blair. See this blog and website featured in my Blogroll to learn more about Julie W. Needless to say-they are both rock star PTs that I really admire, so it was a honor to stand up and speak with them.
Here I am in Talk #2. Credit to Julie Wiebe for the awesome slide. Credit to Jen Miller for the photo.
I was up first. I joked that they were hazing me and made me go first and explain all the “sciency” concepts because I was the baby of the group. For the record-It is NOT easy to speak continuously for an hour! Talk #1 was only 9 minutes. This one took me 65 (apologies to Julie W for being long-winded…I blame the bad video connection!) The good part about having to teach a big group science concepts is I also got to exercise my inner 3rd grade teacher-meets-kids Pilates instructor. Getting a room of 100+ people on their feet and making them wiggle and do some silly things really does give an air of feeling powerful (or maybe that’s just what I’m telling myself).
Audience on their feet, following directions. What fun!
We had a pretty awesome message to share, if I do say so myself. The presentation, Building the Female Athlete from the Inside Out, conveyed the most current ways to build and fashion a female athlete’s movement performance after injury or impairment. We took a multifaceted approach, covering three unique cases. I discussed a young female athlete (my wheelhouse!), Blair shared about a post-partum runner (her true love), and Julie W anchored the relay by taking on the beast of the CrossFit/High Impact athlete (seriously, she is the only person I know who can talk publicly about that hot topic and not get tomatoes thrown at her).
Here I am with the Female Athlete Dream Team: Blair Green & Julie Wiebe. Fully representing The Georgia Bulldogs and Duke Blue Devils in our color scheme.
Of course, this presentation was not without its blessing from Sir Murphy and his law. While I had carefully ensured no encore performance of the computer issues I had in talk #1 (of course I had!), it turns out there were more issues to be had. This happened in the form of the presentation completely shutting down in the middle of Blair’s portion. <Cue potential panic attack>. Good news—turns out we could give the presentation in our sleep and she carried on and handled it like a champ while I scrambled to help her fix the problem.
#nerdclub president takes the podium. Who cares if the presentation shuts down in the middle? No biggie.
Overall in that talk, we had our share of issues and imperfections. There was certainly a laundry list of things to improve upon in the future. Despite those things, the outpouring of support and gratitude following our presentation was humbling. We were tweeted, retweeted, facebooked, Pinned, emailed…the list goes on. As far as social media goes, we were definitely feeling the PT nerd love.
I’ve sat in many talks tweeting stuff the presenter says. Now I’m the one being tweeted. #whoa #humility #carefulwhatyousay
But perhaps the most rewarding feedback we received was at the conclusion of the presentation. As the last presentation on the last day, we were afraid nobody would stick around for our talk. On the contrary, we had a room full of engaged attendees. As we entertained questions from the audience, one attendee stood up from the front row and said nothing, but just began clapping. She turned to the audience and continued to clap, offering up her own personal standing ovation. I was thinking to myself wow, this attendee is quite enthusiastic. Not to mention she has some guts to stand and do that. She then turned to us and said “Ladies, you NAILED it.”
Then she identified herself. It was Mary Massery.
For those of you who aren’t PTs—this would be akin to having Coach K stand up and applaud you as you gave a talk to the entire NCAA on new and innovative approaches to coaching men’s college basketball. Yes, of course I’m going to use a Duke basketball reference after that win over UNC this week.
We were starstruck, to say the least. For Blair and I, both of our jaws immediately hit the floor. According to Blair, this was like being thanked at the Oscars. Julie W knew her previously but it was clear that was very meaningful to her as well. When I was in PT school, I was told by multiple professors that if you ever had the opportunity to learn from Mary Massery-you do it without hesitation.
To add vulnerability to humility—I had even quoted her twice within the presentation, not knowing she was sitting on the front row. This, ladies and gentlemen, is exactly why we are always taught to check and double check references before quoting someone! My 5th grade and high school journalism teachers would be so proud.
Mary happened to escape the room before I had a chance to thank her and shake her hand. Good news is she’s coming to Atlanta later this year and I will get to do that AND learn from her, as recommended to me when I was a novice PT. She did send an email to us later commending us on our effort. It’s not quite a hand shake, but my jaw may or may not have hit the floor again.
Overall, it was a wonderful experience. Among my many reflections, here are a few pearls I picked up along the entire journey:
Like in any sport or activity-you can prepare, rehearse, perfect, and polish to the nth degree-and things will still go wrong. The key? Learning to roll with it and breathe through it. You’ve got this.
Humility, vulnerability, and grace go a long way. It’s not about YOU in sharing your message. It’s about the people with whom you share it. It’s more important to establish a connection with them in order to get the message across than to worry over the details of the actual message. People only retain 10-20% of what you say. So it’s not about what you say-it’s why and how you say it. Be yourself, add some humor and fun—and people will really engage with you. This makes it a lot more fun as the presenter, too.
I say this all the time—but teaching is not a teaching experience. It is a learning experience for the teacher.
Blogging is a fantastic platform for sharing passions and messages. It’s even more fun when you are given an actual voice on an actual platform, and you get to wear heels to do it. Thank you Blair for letting me raid your shoe closet.
The unconditional support, compassion, and reinforcement I received from people who barely knew me was so humbling and validating. It has been amazing to receive messages and emails from people who just want to network and share their stories with me. What an incredible profession to be a part of.
Duke alums in PT gathering! Some of my favorite PTs in the world in this photo!
I’m thankful for the opportunity to have shared my stories and passions with so many people. I can only hope that even just one person has been able to integrate some of those concepts into their daily practice. I gained new inspiration not only for this blog, but reinforced and reinvigorated my curiosity and passion for so many things related to the care of young athletes. As I come down from the CSM high-or hangover as I’ve called it-there is plenty to integrate into my practice. Lots of new connections, friends, and knowledge. I haven’t even started to reflect on all the cool things I learned at the conference in all the classes I took (another post for another day). Stay tuned!
Athletes of all ages and backgrounds thrive on efficient movement, maximizing results with as little energy as possible. In swimming, inefficiency can lead to many injuries, especially shoulder pain. Meet a swimmer’s best friends and mortal enemies. It’s often the enemies—those that pretend they’re friends—who cause the most trouble.
BEST FRIENDS
KISS Principle and the 3 Bs
When it comes to swimming efficiency, we need to establish two simple truths for keeping it simple, swimmer (KISS):
Truth 1: Swimming is not all about the arms. You may have lats (“swimmer muscles”) of steel, but they do more than propel the body in water. They interconnect with the core and are sewn into your glutes. The arm bone is connected to the leg bone after all! But that doesn’t mean it has to do all of the work. Truth 2:Swimmingisall about the 3 Bs: balance, buoyancyand breathing. But how do you make those your best friends? Read on to find out how to use them to help your arms and swimming efficiency, specifically in the freestyle (front crawl) stroke.
Be strong and carry a big kick
“I am not a strong kicker” and “I hate kick sets“ are common quotes from swimmers with shoulder pain. We may love-to-hate kicking, so let’s make it more digestible with a metaphor. Imagine you have a beautiful boat that you use each week. You’re thrilled until one day—BAM! The boat starts to slow down and feel sluggish each time you take it out. You take impeccable care of your boat, so you’re baffled. You take the boat to a mechanic, who asks how you drive it. You proudly present two paddles that you hand-carved. He smiles and points at the boat’s motor. “This is a motor boat,” he says. “Have you been paddling it all along?” You answer, “Yes! I don’t want to pay for gas and put in the time to service the engine!”
Friends don’t let friends overlook the importance of having a strong motor in the water. Using your “paddles” to do all of the work is not only inefficient, but it will slow you down and worse—potentially injure you. Dragging your motor along is added weight for your arms to pull. Use that weight to your advantage! Find a precisely balanced use of that motor coupled with good body rotation (twist), balance, and buoyancy so that you won’t have sore “paddles.” Want to know more? See this article about efficient freestyle kick in swimmers and triathletes.
Do the twist
There is no one-size-fits-all answer to swim posture and balance, but here are a few guiding principles:
Head position: Head position and shoulder pain are related. Poor head posture begets a sluggish hip position and vice versa, leading to a sluggish motor. Gaze through the top of your goggles instead of tilting your head up. Keep the water line at mid-forehead or cap line.
Pelvis and hip motion and rotation: drives the kick, which in turn drives the body, then the arms. This requires glute and hamstring strength and flexible hips.
Upper back: follows the pelvic and motor motion. You need flexibility and strength into twisting motions in the upper/mid back, shoulder blades, abs, and low back.
Knees and ankles: neither held too rigid nor floppy. Kick from the hip, not the knees or ankles.
Utilize your own personal floatation devices
If you don’t breathe well, your motor and 3 Bs will suffer. Swim lessons begin with bubble blowing and floating for a reason: to teach use of the most buoyant part of the body—the lungs—to stay afloat. Diaphragmatic breathing keeps your core engaged with your arms and delivers oxygen to your muscles. And be an equal opportunity breather! Breathe bilaterally to keep the work balanced on each arm/leg.
Swim toys: the good guys
Swimmer’s snorkel: Ditch the nose plug. The swimmer’s snorkel may help you with the 3 Bs. It keeps your head and body in line while working on your body rotation and kick. Sure, you won’t breathe to both sides or compete with it, but it does help you sync your inhales and exhales with your strokes. That’s a step toward 3 B success and a best friend for swimming life!
Swim fins: Not only will they help you practice your Little Mermaid impression, but swim fins will also help you run over everyone at practice. While they are no replacement for establishing an efficient motor and 3 Bs on your own, they do boost kicking and, in exchange, take a load off of your arms. Word of caution: if your ankles are stiff, they can cause shin pain.
Hand entry
It’s easy to get caught up on hand entry (pun intended). It’s important, but not everything. Hand entry is akin to a runner’s foot strike: both are dependent on body position. This has less to do with your arms and more to do with—you guessed it—kicking and the 3 Bs. With these in check, the hand should enter fingertips first, just wider than the shoulder. Too wide or too narrow likely means there’s under- or over-rotation in the hips and torso, respectively. This can lead to technique issues and stress the shoulder.
Training terrain
This is mainly applicable for triathletes and open water swimmers, though pool swimmers can benefit from this part, too. Just as trail runners need to train off road and road cyclists need to train on the road, swimmers need to train in their competition “terrain.” Accessibility, weather and water temperature pose a challenge here. For open water races, train where you can’t see in front of you. Vision affects the 3 Bs, so practice lifting your head too look for race buoys, support crew, and other competitors. Just remember keeping your head up too long will affect your 3 Bs and motor. If a current or waves are involved, train in choppy water. Wear your wetsuit before race day to ensure fit, comfort, and no change in your 3 Bs.
MORTAL ENEMIES
Improper FITT
That’s not a spelling error, and I’m not referring to swimsuit fit. That’s training Frequency, Intensity, Type, and Time. Too much or too little of each can be problematic. Periodic muscle soreness is normal, but should taper with experience and improved technique. Increase training distance or duration by no more than 10-20 percent per week and vary your strokes to allow for this gradual change. Having stroke variety (e.g. breastroke or backstroke) in the back of your Speedo can be handy if you need to change your position or speed in a race.
Swim toys: the bad guys
Kick boards: Kicking is essential to healthy shoulders, but kicking with that 12-inch piece of foam is not. It puts the shoulder in the “impingement” position, pinching your rotator cuff and other structures against your scapula. That’s PT-speak for “ouch.” Kicking with no board helps master the 3 Bs. Kick on your side with one arm up or on your back or stomach with both arms down.
Hand Paddles: These are a privilege, not a right. Added resistance is great for building shoulder strength and to the swimmer who paddles the motorboat. Remember what I said about the arms? It’s not about them! Unless you have no pain, a good kick and the 3 Bs, just don’t even go there.
Pull buoys: Why would you take away your motor especially when your shoulder hurts?
Poor ergonomics in other activities
What you do out of the pool is just as important as in the pool. Poor cycling and running posture can beat up a shoulder. That goes for workplace, school, and car ergonomics, too. Habits accumulate quickly and can catch up to you when you least expect them.
IN SUMMARY:
Now that you’re armed with a checklist, you’re ready to dive in and make lots of new best friends. But if you find you’re having trouble with them, don’t wait until you’re in pain to ask for help. Sports physical therapy is not just for when you’re broken. We can identify factors that may put you at risk for injury not only in swimming, but in other activities too. Video stroke analysis can be key to help identify and correct errors that may strain a shoulder.
“Hey, do you know of any places where my daughter can do Pilates after she is finished with PT?”
“Should my 6 year old do Pilates classes?”
“She has a stress fracture in her back and the doctor said she needs to strengthen her core. I heard Pilates is good for that so I bought her a DVD. Is that ok?”
“I need to do Pilates as conditioning for dance. What should I do?”
I get these questions all the time from parents and young patients. My answer to them has often been “Well it depends.” That is, until recently!
One month ago I had the absolute joy of attending the Pilates Method Alliance® Pilates 4 Youth teacher training in Berkeley, California. What a fabulous 2-day course in the most beautiful setting with the most interesting and brilliantly creative minds!!! It was perhaps one of the most inspiring courses I have taken in my entire PT and Pilates career thus far. It helped that we had a nice view of the San Francisco Bay, San Francisco, the fog, and the Golden Gate Bridge the whole time. I called it my #nerdcation.
Claremont Hotel & Spa in Berkeley.
I’m not sure if I spent more time learning or more time gazing out the window from my seat
The course was full of 60 or so instructors from all over the USA and the world who work with children and adolescents in all different settings: schools, clubs and camps, inner city wellness initiatives, health care/PT clinics and private practices, girl scout troops, and private Pilates studios.
The course was led by Celeste Zopich, Brett Howard, and Dawn-Marie Ickes, who co-authored the course manual and textbook Pilates for Children and Adolescents. These three brilliantly creative master teachers spearheaded the Pilates in the Schools movement, an initiative begun in the early 2000’s in the wake of decreased physical education time in public and private schools. You can read more about Pilates in the Schools and the research project they did with the kids here.
Watch a video about Pilates 4 Youth & Pilates in the Schools here:
I can’t say enough good things about the instructors. Celeste has a wealth of experience teaching in a parochial school. Brett teaches classes for children of all ages and brought a wealth of research and creative cueing and activity design perspective to the group. Dawn-Marie, the PT & Pilates teacher of the book, seems to be leading a life rather parallel to mine on the west coast. She works not only with young clients and incorporates Pilates into PT with them, but also has a special interest in women’s health and is a Redcord Neurac teacher trainer. I can’t wait to continue following these three as the Pilates 4 Youth initiative continues to take off.
See interviews from the book’s authors & course instructors here:
Too often children (especially girls) drop out of sports by age 13 due to burn out from early specialization, self esteem and body image issues, lack of success and fear of failure, or lack of funding from parents or other guardians. Or—on the other hand, children do not become active in the first place for so many cultural and societal reasons (that I don’t have time to discuss in this blog post) and we have even bigger problems of childhood obesity, low self esteem and body awareness, and low exercise interest or confidence.
Perhaps most interestingly, the course taught us about the “magic window” age of 9-13. This is when kids and teens are at the most vulnerable for both physical and psychological injury. The mind-body approach of Pilates targets these problems in a very kid & teen-friendly way. This is the best stage to intervene from an injury prevention standpoint in PT, too.
Favorite video quote from videos above (from a 13ish year old):
“Well I’m a swimmer and doing regular Pilates has helped me a lot with having regular breathing and opening up my shoulders and using my back muscles to move my arms.”
If that quote doesn’t sum up my personal and professional vision for helping my most beloved target clientele, I don’t know what does.
In the course, we learned how to design classes or private sessions for children of all ages and ability levels, from 5-6 year old girl scouts to 18 year old elite Olympians,. We had a great segment taught by Dawn-Marie on program design for children with special needs, or “special opportunities” as she liked to call it. She reminded us that all children and teens have challenges that vary on a long, diverse scale, regardless of the diagnosis or “category” in which they are placed. For youth of all ages and ability levels, it is our duty to determine how best to tap into each of their movement systems, regardless of the challenges and opportunities they face each day.
Superhero themed Pilates! It’s not hard work when you’re having fun while learning! I bet I know a few adults who would probably want to come to a class like this one…
The Pilates 4 Youth initiative is in a pretty grassroots stage now. So far the course has been put on twice to a total of about 150 people thanks to a grant from a generous donor. Hopefully it will continue to grow in popularity so that we can improve access for children of all ages to Pilates in a non-competitive environment. But we’re not exclusive to Pilates. And we are all over social media!
#hashtags are everywhere Follow the PMA on twitter at @PMATWEETER
Stay tuned! I’ve already been incorporating Pilates into my clinical practice for several years, but I’m anxious to start incorporating many of the new concepts I learned into practice and hopefully into group classes in the community soon. I’m excited to exercise my creative juices and have already invested in some fun tools to help me do so:
That’s a scooter board
Fabulous imagery and kid-friendly Pilates terms
To learn more about the Pilates 4 Youth initiative, check out the information on facebook.
Just ran across this great whiteboard video from an NPR post about low back pain. It’s a video by a Canadian primary care physician. It’s the best patient-friendly explanation I’ve seen of low back pain, what to know, and what to do about it.
While low back pain in the young athlete is not always the same as in adults and there are other kid- and teen-specific diagnoses AND PT treatments to consider, I still find this video very helpful for all ages. Though there are some very rare reasons they may have it, kids and teens almost never have problems like neurogenic claudication due to spinal column narrowing mentioned in the video. Discogenic pain is also more rare in kids and teens..
Given that low back pain is one of my favorite conditions to treat, particularly in the young athlete, I’d say this video hit the nail on the head for the most part. I love the physiotherapy, manual therapy, and Pilates shout-outs in the video. It’s important before beginning something like Pilates or yoga that you start slowly and ensure that your instructor is familiar with how to help people with injuries. In addition, if you are a kid or a teen, it’s important that the instructor is skilled in working with children and adolescents as there are special precautions that must be made in Pilates and yoga due to differences present in the growing spine vs. the adult spine. Typically what I do, as a Pilates instructor and PT, is teach kids the right movements they would need to know for Pilates, then find them the right Pilates instructor or class.
You can skip the ad at the beginning, but I also love the Neurac and WebPT advertisements at the start of the video. Between Pilates, Neurac, and WebPT, I use all of these things in my daily practice (in full disclosure: nobody paid me to say that).
The best 3 lines:
“Motion is lotion”
“A physiotherapist can probably help you with all of these things”
Last week I saw this Always ad defining #likeagirl. It went pretty viral among my facebook and twitter circles. If you didn’t get a chance to see it, see the link below. If you did, it’s worth another watch.
Upon watching this, I found myself wanting to cry, scream, smile, laugh, and fist pump. My personal and professional worlds were colliding. I love kids. I love psychological development (it was my major). I have studied peer relationships of children and teens. I love young athletes (it’s the title of this blog). I love a good youtube video and I love social media. I love advocacy for women’s health issues across the lifespan.
Like in the video, I wondered who is defining #likeagirl and why it is viewed by so many as an insult, especially when it comes to young athletes. Where did all of this come from–is this a thought women have of other women? Or a thought men have of women? How did girls’ own views of the phrase #likeagirl spin 180 degrees from positive to negative in a just few years across the young female lifespan?
Like any deep thinking blogger, I of course thought “this would make a great blog post.” I began to reflect on some striking #likeagirl challenges in my own upbringing as a female and how it affects my thoughts and views on this idea.
#Likeagirl defined during the “growing up” years
In 4th grade, I was one of only 3-4 girls in my class. I was teased, bullied, and outcasted for being the only member of the class in the gifted program. Anything anyone could try and take from me, they would. Lunch, pencils, erasers, paper, sanity, innocence…you name it. We tried to get the teacher and school to intervene but nothing really changed. So, fight #likeagirl I (well, my parents and I) did, and I moved on to a different school.
In 7th grade, the most “popular” girls sat next to me in science class. I specifically remember my “friend” asking me if she could cheat off of me during tests. I said no. There went that friendship. Apparently the way to popularity and being accepted #likeagirl was compromising morals.
As we walked down the staircase toward our 9th grade geometry class, my friend said “You know if you keep it up at this rate, none of the boys are going to like you.” It was me making straight A’s, swimming 5 hours a day, and setting nearly every school swimming record.
My friend then followed with “they’ll think you’re intimidating. Boys don’t like intimidating girls.”
At the time I remember thinking “wow, that sucks, boys won’t like me” for about 2.5 seconds. Then I was mad at her for thinking that saying that to me was going to change who I was and make me “give in” to the female norm (whatever that was) just so that boys would like me.
As if my friend were a fortune teller, I didn’t have a boyfriend for 3 years after that. That’s eons as far as high school goes. I had my moments of insecurity about it, but had plenty of other things going for me to distract me. I wasn’t worried about finding Mr. Right at 14, 15, 16, or 17. Ironically, I found him at 18. Mr. Right will tell you that he wasn’t intimidated by me, but looked up to and was inspired my successes. We started dating a month before high school ended. We’ve been together since then and now we’re married.
Daniel & I at our wedding in 2009. Duluth High School Class of 2002 representing!
Take that, Mean Girls.
Growing up, I was too busy swimming to get bogged down in the details and drama of teenage life. Being surrounded by a team that fostered friendship, acceptance, self discipline, self-confidence and the ability to rise from failure is an immeasurable benefit of youth sports teams. Unlike “throw #likeagirl” and “run #likeagirl,” there was no concept of “swim #likeagirl.” We trained in the same lanes as the boys, often pushing each other during practice to help each other improve.
That’s not to say I wasn’t an emotional, annoying teenager (sorry Mom and Dad) and that I didn’t have my moments of being challenged by the #likeagirl norm. I’m also not saying that every girl has to be a competitive athlete to have these values instilled in them. In fact, I believe just the opposite. There are countless other non-athletic outlets and avenues for girls to be successful and gain self confidence and self respect. We, as a society, need to embrace and encourage that.
Defining #likeagirl in the most educated circles
Along with sports, not every female needs academic success to define her, either. You may be surprised to know that even in the most educated circles of women, there are still struggles to define what #likeagirl means.
In college I was surrounded by new ways of defining female success. I’m not sure that I could have picked a better place to foster the #likeagirl mentality. But even Duke harbored its own challenges for women.
I remember walking around East Campus my freshman year thinking “why do these girls all carry purses with a big F or C’s on them? Who is Lilly Pulitzer? And who actually gets dressed in all of that stuff for an 8 AM Chem Lab when you have to wear a lab coat and goggles anyway?” I was completely flabbergasted with the materialistic side of all of the women around me. I had never been around so much privilege and entitlement. Feeling the “sink or swim” pressure, I accepted that I didn’t have to be just like them, even though I did gain an appreciation for things like Tory Burch shoes.
Let’s be honest, materialism is everywhere, not just at Duke. What I found more overwhelming than that was the fact that every female sitting in class with me was somehow like me. Everyone graduated in the top 1% of their class, made ridiculous SAT scores, was an incredible athlete, was devoted to community service and had already published books about it, was going to be the next Maya Angelou or rocket scientist…you get my drift. It was intimidating, impressive, and inspiring.
Here I was, surrounded by successful, accomplished women. I’d yearned for that given I’d run into problems with the definition of #likeagirl success in elementary, middle, and high school. I’m thinking “yes! finally people who are like me who will accept me!.” But something was still missing. I was a nerdy female athlete who liked to wear dresses and pearls one day, do crossword puzzles and hike the next day. This challenge to fitting in to the #likeagirl norm became abundantly obvious to me during sorority recruitment. Like in middle school, these women went to great lengths to be accepted into the most “popular” groups. Sometimes at the sacrifice of their own strengths and morals. That just wasn’t who I was. Also like in middle school, I did not sacrifice my standards to be popular. This was a blessing in disguise. I ended up being president of the sorority I joined, which was a phenomenal leadership and networking opportunity. In my group, women went on to become accomplished and successful lawyers, physicians, published authors, Teach for America leaders, CEOs, Miss America pageant contestants, Peace Corps and military officers, and stay-at-home moms. In our group, #Likeagirl took on many definitions of “awesome”, and that was ok.
In a men’s basketball-dominated school, the leaders of Duke Panhellenic sororities got together to support Duke Women’s Basketball. Our shirts said “Duke Women’s Basketball: the greatest thing since sliced bread.” We even got a notable men’s basketball player to join in our efforts.
#likeagirl challenged by Duke Women’s Initiative
While I was at Duke, these #likeagirl challenges played out before me on a daily basis like a great soap opera drama. It wasn’t just obvious to sorority women. Some smart Duke researchers caught wind of this, too.
The Duke Women’s Initiative was rolled out by woman President Nannerl Keohane in 2002-2003. It was a research initiative raising awareness to issues faced by women at Duke-women you’d think would have no problem defining or championing their successes. It highlighted the juxtaposition that the same women who were some of the most talented in the world in their fields would also find themselves downplaying their success by submitting to disillusioned social norms. They often gave into social pressures to build and mend their developing and broken female egos, respectively. In a sense, there was a real problem among Duke women to define what #likeagirl meant. Being around during this initiative is exactly why I chose to major in developmental psychology with a special focus on development of peer relations, particularly passive aggressiveness among females. I was so curious to know why we as girls act the funny ways we do.
The initiative coined the phrase “effortless perfection.” This describes the amount of effort many of these talented women put in to appear as if they’d put no effort into being successful. Why were they ashamed of people knowing they worked hard or were total nerds? Women confided that they didn’t want to make it look like they’d worked hard to achieve their successes, because hard work and determination connote “male”-like qualities they thought would be intimidating. And really–what it came down to–they wanted to appear this way because they were worried about acceptance and relationships with males and females on campus.
Whoa whoa whoa. That’s kind of like when my 9th grade friend told me boys wouldn’t like me for being successful, because that was intimidating. Or my 7th grade “friends” not liking me because I would not let them cheat. Or being bullied in 4th grade for being the smart girl.
#Likeagirl challenges extended to body image and social success too. Duke women would go to great efforts to mask eating and psychological disorders behind guises of normal-appearing, almost reckless or “laid back” behavior. You’d have the summa cum laude chemistry major who partied every night with her friends, but never studied with her friends because she didn’t want people to know she spent 10 hours/day in the library to get a 4.0. She only wanted them to see that she was a “cool party girl.” She probably didn’t like to talk about her grades or successes.
Like her, many women didn’t want men or other women to be intimidated by their efforts at appearing perfect, so they often hid those efforts or behaved in polar opposite, sometimes reckless ways. They didn’t eat or exercise with others for fear people would see how hard they worked to remain thin. They didn’t want to appear aggressive and dominating or weak and vulnerable for fear that they would not find friendship or intimacy because of those things. So we didn’t want to appear aggressive or intimidating, but we didn’t want to appear vulnerable either. Whew. Make up your mind, ladies!
On the swim team, there was no hiding how hard we worked or how much we ate. We all trained together, ate together, and often studied together, supporting each other through all of our efforts to be successful. This is my friend Julia. Julia was a Rhodes scholar finalist who went on to Harvard law school. Now she’s a rock star lawyer in Chicago.
As much as we did not or do not want to admit it, all Duke women likely had a piece of this mentality in us. After all, I’ll bet several of those women were 9th graders who were told it was not “cool” to be smart or successful. Why else would we, as a cohort, mask our successes in “effortless perfection” to try and fit in?
It wasn’t as bad as it sounds, though. There were great things about being around so many smart, successful women. I was fortunate to live with a different woman each year. Each woman had her own unique background and definition of #likeagirl. One was a varsity athlete, another was a biomedical engineer. One was a former pageant contestant, Duke cheerleader, brilliant double major, international public servant and future rock star pediatric NICU specialist. One was a champion of all things liberal arts, challenging abstract and socially responsible thinking on a daily basis.
Duke psychology majors. The blonde at the far right of the photo is my freshman roommate, Katie. Katie is now a lawyer. The girl on the left side of the picture is my sorority sister, Claire. Claire did Teach for America and now works as a science teacher.
These girls all had one thing in common: like me, they all had their struggles with defining what #likeagirl means. But they also didn’t let their athletic, nerdy, or “intimidating” pursuits get in the way of their relationships with significant others or friends. They didn’t compromise their personal standards so that “boys or friends would like them.” And they didn’t hide their efforts in being successful. We didn’t compete, but challenged each other. We were ALL far from perfect and accepted each others’ effortful imperfections. We were proud of being successful women without feeling shame for it. Maybe that’s what #likeagirl meant to us and should mean to everyone else.
The girl in the boot is my junior roommate, Kaitlyn. My sorority sister and good friend Becca is at right. Dr. Kaitlyn just completed pediatric residency. Dr. Becca now has a PhD in clinical psychology.
Defining #likeagirl in the professional world
In physical therapy school, I continued to raise the bar for myself. I didn’t make straight A’s and get uber-involved because I cared about the 4.0 or what involvement would look like on my resume. I did these things because, after all, this is the profession I chose to do and was paying a lot of money for. People were going to be trusting me with their injuries and their lives…and paying money for that! I wanted to soak it all in, then continually grow and learn more.
That’s pretty much what I’ve done–and I’ve done so following in the footsteps of some other PTs who totally rock it #likeagirl. Read this keynote address for incoming PT students last year given by one of my PT mentors who also happens to have founded the practice where I currently work. She has a great message of fighting #likeagirl to overcome adversity, embrace change, challenge the “norms” and become successful. She mentions the idea of surrounding yourself with people who are better than you are, surrounding yourself with people who challenge you, and taking in as many professional development opportunities as you can. Never does she mention compromising your values because “it’s not cool to be successful.”
I love what I do and I love learning more. I keep finding new things to learn about and courses to take. And now-I love teaching about it too. I have the privilege to teach students in the clinic and teach in the same PT program from which I graduated. I’m surrounded by fascinating female (and yes, some awesome male!) colleagues to keep me driven.
Nerdy PTs, mentors, and mentees have fun together. Here is part of the #pelvicmafia, a grassroots group of rock star women PT leaders advocating for awareness of women’s health needs all over the globe.
Recently, along with some awesome PTs, I was invited to share my nerddom with other PTs by teaching at next year’s national convention. It’s completely intimidating, but in an inspiring way. But, to be honest, I don’t need a convention to share my excitement for what I do. In my own life, I’m retweeting, sharing, pinning, instagramming or posting every article or inspirational item I can find. To all of you who follow me—sorry I’m not sorry for bombing your newsfeeds and timelines with this stuff.
Nerdy PT posts dominate my twitter and facebook feeds often accompanied with #nerdclub
#Likeagirl, I’ve turned from the girl being bullied or shamed for being nerdy and successful to someone who is proud to own it. It helps that I have a few supporters who are proud to “own it” with me.
Nerds can be princesses or Wonder Women, too. Here I am with the #nerdclub president.
#likeagirl, Dr. Julie style
And now I find myself colliding all of my passions, specializing in and working with young athletes. Working with young girls from age 6 and up, I have the joy of seeing girls go from “cute” and running #likeagirl in elementary school turkey trots, “sassy” and competing #likeagirl to make the middle school cheerleading squad, to “sophisticated” and swimming #likeagirl in high school to set records. I’m just happy to help them explore and stay strong in their passions and dreams. Unfortunately, along the way I’ve seen my fair share of girls who have fallen prey to peer pressure and given up on the dreams they’d once devised for themselves at that cute, turkey-trotting age.
My favorite 6 year old: being a rock star cheerleader
The most common age for sports dropout is 13. It’s that “magic window” age when girls are in that 7th-8th grade world of “to give in or not to give in.” Unfortunately in our world, there aren’t other great activities that are always “acceptable” for girls to put their hearts and minds into. Though I imagine there are exceptions to this, girls who hang out with the geeky boys, are in engineering club, beta club, national honor society, robotics club, and the 4H club—but don’t play sports or do “girly” things– likely won’t get elected to be prom queen.
And that makes me sad. I’m not saying the traditional “girly” or “sporty” things are bad. Be a pageant queen! Be a princess! Be a star athlete! Go you! I’m also not saying that the 4H club president needs to be famous. But girls need credit and encouragement for more than the traditional #likeagirl roles they have been given. They shouldn’t have to become “effortlessly perfect” for fear that someone will think they’re intimidating, nerdy, or not feminine for being successful.
She may not know it yet, but my favorite 6 year old is also the president of the junior #nerdclub
See this fabulous video from GoldieBlox, a company and campaign devised to inspire girls AND our culture to balance, nuture, applaud, and respect girls’ interests, regardless of what they may be. When I saw that video, it took me back to more of my college observations about defining women’s success by more than just a gender role.
In my experience as a youth sports PT, I find in that “magic window” age of 10-14, too many girls show up on my caseload riddled with pressures placed on them for being too athletic or not athletic enough, too nerdy or not nerdy enough. Some have injuries that just won’t go away without a medical explanation for them. It’s no secret to many of the professionals with whom I work that the girls are often subconsciously using their injuries as an “out” from the pressure of sports. As long as they are injured, they don’t have to compete. Plus they get a lot of love and attention by way of parents, friends, and healthcare professionals worrying after them and making them feel special. It becomes an endless, often sad, cycle, that can end in being socially outcasted, or in medical complications including anxiety, depression, and general decreased conditioning because they are no longer exercising. I think we can all agree that overall these situations probably aren’t the most productive or positive ways to make the girl feel special and valued.
It’s my wish in working with young female athletes or non-athletes, that they never feel pressured to stay involved in a sport or activity that doesn’t make them happy. Likewise, she should be accepted for doing the things that do make her happy. If a girl does or doesn’t love an activity, she should live in a world where she feels ok saying so. She shouldn’t be shamed for being successful because “that’s intimidating.” That can backfire, too. She’ll give up on her dreams and eventually get herself into trouble in some way. Even the young athlete who loves her sport should be encouraged to find balance in her interests, to find success in more than just her sport, academics or her appearance.
It’s important we as a society (and medical profession) encourage success and self confidence in any interest a girl has. We need to encourage that #likeagirl means something awesome, not awful. Maybe that 8 year old princess-loving girl will become a beauty model or Hollywood actress. Awesome! Good for her! Or maybe she will be the CEO of a Fortune 500 company. Or perhaps she will design the next vehicle that takes humans into space. See this GoldieBlox video about women becoming engineers.
Developing girls are vulnerable. What we as adults say to them makes a lasting effect. What their peers say to them makes a lasting effect. Just notice how vividly I remember 16 years later when my friend (who is still a good friend) said to me how unpopular or undesirable I was going to be for being a successful female.
So please—no matter what inspires her—help your daughter, sister, niece, friend’s daughter, friend, student or patient have the confidence to be proud to be #likeagirl, no matter what she does to succeed. Help her be proud to humbly share with others how much effort she put into doing so.
Model positive behaviors. Service, encouragement of other women, making friends with boys without making them boyfriends.
Encourage healthy competition on things that should be competitive (which is almost nothing we do). Encourage teamwork, compassion and support on everything else (which is almost everything we do).
Help her learn the difference between “humility” and “weakness”.
Help her learn the difference between “aggressive/intimidating” and “assertive and motivated”
Define success and confidence in something other than trophies, first places, makeup, number of boyfriends or girlfriends, or the size of her bra or her pants.
Help her learn that she does not have to strive for perfection in anyone’s eyes, not even her own. Flaws and differences are good, too. If she is that successful girl (which she will be if you follow all this blogworthy advice), let her know it’s ok to show and be proud of how much effort she put in to that success.
It’s ok to be different. Help her embrace the things that inspire her and make her unique, even if you don’t necessarily find yourself inspired by those things.
Encourage her to fight #likeagirl in whatever area inspires her and not let her gender define her in any way.
Step it up ladies! You don’t have to be a muscle bound, Rosie the Riveter type to be #likeagirl. It’s ok to be a pageant superstar, a cheerleader, or a princess. But it’s also ok to be an aerospace engineer, high powered CEO, blacksmith, NFL football coach, farmer, or construction worker. Be proud of who you are and model a positive female outlook for all those girls who are looking up to you. If you think someone looks “weak” just say so. If they look strong or successful, just say so. It doesn’t have to be tied to gender roles. Let’s make #likeagirl mean #likeawesome and not #likeawful.
Physical therapists have a vast toolbox of skills to help improve someone’s ability to move. Within that toolbox may be exercise techniques, Pilates, Redcord Neurac, dry needling, other manual therapy techniques, taping, tapping, yelling, cheerleading, lecturing, parenting, inspiring, and mentoring. The truth is, despite what any studies say or any expert will tell you, there is probably not ONE best treatment for any young athlete. I will say no more because Adam (@thesportsphysio) who I follow on twitter really just summed it up best. I’ll let him do the rest of the talking…
As a physical therapist practicing in Georgia, I have the privilege of being able to use the skill of trigger point dry needling to help patients with myofascial pain and dysfunction, joint stiffness issues, acute and chronic injuries, tendon problems…the list goes on.
Working with a majority of younger patients, I often get questions like “Do you dry needle kids? What’s the youngest patient you have needled? Will my 10 year old benefit from needling like I have?” Those are all good questions. Before I answer them, I think we should cover a little background on this whole needling thing.
What is trigger point dry needling?
In a nutshell, dry needling is a form of manual therapy where the physical therapist or other trained practitioner inserts a solid filament needle into a trigger point in a muscle. This may stimulate a local twitch response in the area, creating a cascade response that ultimately results in a release of the trigger point…or at least that is what we believe happens.
While there is growing evidence for the effectiveness of trigger point dry needling and several studies on what is happening during the technique, the reality is that nobody knows exactly what happens during each treatment in each person. We just know it works and have seen it work time and time again. We believe that the response may be chemical, neurological, mechanical, all of the above, or some of the above. This may vary from place to place between patients or even in various locations within the same patient. Or perhaps it’s a higher order sensorimotor experience change in the brain’s cortex–which I suppose would technically be all of the above depending on who you ask. Either way, there can be great changes that when used in adjunct with other physical therapy tools, pave the way for the patient to see outstanding functional changes.
If you’re still not sure what dry needling is, I recommend you visit these websites for some information:
Is dry needling the hot new thing in physical therapy? Why have I never heard of it?
In some places and in some schools of thought—yes or no. In the grand scheme of the constantly-evolving practice of physical therapy, dry needling is the new kid on the block in many states and in many areas of PT practice. You may not have heard of it because while most physical therapists possess the skills to do it, not all 50 states allow them to do it yet.
What physical therapists can perform trigger point dry needling?
Currently, dry needling requires advanced training beyond the realm of entry-level doctorate level physical therapy education. It is recommended that new graduates wait a year or so to begin training in this practice as good performance of dry needling requires more advanced skills. While new graduates have many excellent skills, the decision-making and safety behind dry needling takes extra time to develop the “finesse” of performance.
Is dry needling the best physical therapy treatment out there?
That is all a matter of opinion. But generally-the answer is probably that there is not one BEST physical therapy treatment out there. Don’t get me wrong-dry needling is one very helpful tool for many patients, but it is not THE tool. In states where dry needling is not legal for PTs to perform, patients see great results with a plethora of other treatment options. Not being able to perform dry needling does not make a clinician any less skilled; likewise, being able to perform dry needling does not necessarily make someone more skilled. It’s just an additional skill to add to the “PT skill toolbox.”
What’s most important are the “above the neck” skills of decision making, assessment, clinical reasoning, and finding the BEST treatment option for EACH patient that allows him or her to optimize the ability to move. See great recent blog about this here. This ability requires a good balance between manual therapy/dry needling, functional movement assessment and re-education, strengthening, stretching, and the good old fashioned teaching and learning interventions my patients lovingly call “Julie’s Sermons.”
So now that we’ve established what it is, where it is, who can do it, and how it fits into PT practice, I can move on to the question I know you’ve all been asking…
But Julie…do you needle KIDS?
My answer is usually something along the lines of “Well, it depends on your definition of kid.” See my first post in this blog to understand my definition of kid. Some “kids” are 44 year old elite athletes who cry like babies when I so much as mention the word “needle.” Some kids are 11 year old elite gymnasts who come in begging for needling and swear it is the one thing that keeps them competing at Level 9.
In general, I tend to look not at chronological age, but a plethora of other contributing factors. This requires the need to use all of my senses to determine just who is the right candidate. One could argue that this rule applies to any patient of any age. Chronological age is one factor. Other factors include emotional stability, emotional and cognitive maturity, education level, personal pain experience, activity level, overall/general health, and tendency to faint or scream at the topic of needles.
So, it’s complicated. If you’re looking for an age “limit” recommendation on dry needling, you’re reading the wrong blog. What I can definitively tell you is maybe you want to steer clear of the super young children. Maybe under 6. Then again, I’ve heard from colleagues that it’s been done on younger kids before, as have trigger point injections performed by some of my physician colleagues. It’s just not black and white.
What I can also tell you is that as of this blog posting date, the oldest patient I have needled is 82 and the youngest is 11.
See this resource from a few pediatric and adolescent sports medicine experts on the practice of dry needling in this population.
Let’s dissect a few of these factors to determine which kid is the right needling candidate.
Emotional stability and maturity
I am not going to lie to anyone. Dry needling can be a little uncomfortable. In general I find that anyone who is not in an emotional place where some discomfort can be tolerated may not be the best candidate. On the other hand-some patients can be fearful of movement/exercise and prefer the security and relief that needling brings after treatment, despite discomfort. Sometimes it’s just emotionally easier when passive treatment is performed on them. They can get a little emotionally attached to the technique. This can be a problem too.
Kids and teenagers—and even adults–can be afraid when it comes to medical interventions. Fear and anxiety can sometimes improve with some coaching and the patient will eventually agree to try dry needling. Others are totally emotionally on board, and then it maybe didn’t live up to their expectations—so they jump ship and ask to not have it performed again. See what I mean? It’s complicated.
Cognitive Maturity
“Wait so, you’re telling me this may be uncomfortable. Remind me again how doing something that’s uncomfortable is going to make me feel better?” To some kids, particularly younger kids—this concept is not even an approachable topic of conversation for me. From a cognitive maturity standpoint, some kids just haven’t developed the ability to discern the “later” benefit of doing an uncomfortable “now” treatment. I general I see that in many kids this improves from age 9-11. But then again-it really just depends on the kid.
I also find—and this is my TOTAL anecdotal experience—that sometimes the more the parent is on board with the kid having the technique done, the less the kid is willing to try it. There are many exceptions to this. Some kids and teens do exactly the opposite of what the parents recommend. Most parents would probably agree this concept isn’t exclusive to physical therapy sessions! In other cases, the parent says “poke him” and the kid says “let’s do it!”
But—I use some definite discretion here. Bottom line: I have a strict rule that I must get a resounding YES from the kid or teen before I glove up and pull out the needles. An “I guess” or “Whatever my mom says” just won’t cut it. Sometimes it takes kids a few sessions to warm up to it. Sometimes we try it and it doesn’t really seem to help—largely because I don’t believe they truly understand what I’m doing. The good news is we have so many other interventions we can use that sometimes we don’t even need to go through with needling.
Education level
It’s important any patient be at an education level that they can understand the basic concepts of benefits, risks, alternatives, and outcomes required of an informed consent. Generally, most kids at about 8th or 9th grade can handle a mature discussion on the pros and cons needling without a lot of parental intervention.
What I find often is that the patient who is not WELL educated on medical procedures, but ALMOST well educated is the biggest threat to dry needling candidacy. These are kids who are super smart and have done a little research on their own. Perhaps they have consulted Google, their high school anatomy class, or just talked to friends. Needless to say—they thought that because they knew the name of one muscle in the vicinity of their injury or pain, that it MUST be the muscle that needed to be dry needled.
And kids can be very black and white about it—believing dry needling is the only thing that will fix it. Kids can be very smart, but let me remind you about cognitive and emotional maturity. They generally don’t develop their higher level processing and abstract thinking skills until late high school, college, or even mid adulthood. Some people never develop it. So they firmly believe that putting a needle in the muscle will immediately fix their problem that has been going on for months.
Anyone who knows me knows that this is not quite how I operate, nor how I believe humans operate. I am not a one-and-done type of physical therapist. I get down to the source of WHY that muscle is affected due to how the patient moves or how the patient believes he or she should move. Address that first and see if the trigger point is still there later. Then we’ll talk about putting needles in the serratus posterior inferior. Yes, someone asked me to specifically do that and no, I’m not trained to put a needle there.
(End rant)
Personal pain experience
Someone call Lorimer and David. They can explain this part way better than me, but I’ll take a stab at it (pun intended). I could probably go on for days about how a person’s experience with pain is highly individualized. Some people get a hangnail and it is the most painful thing they’ll ever describe. My good friend just gave birth to a nearly 9 pound kiddo without the use of drugs or any intervention. She didn’t say it wasn’t painful, but she certainly lived to tell about it with a smile on her face. I’ve seen 15 year olds burst into tears when I told them I was not going to needle the tiny knot in their back muscle because I did not believe it would be beneficial.
Pain is emotional.
Pain is an output from the brain. See this post to explain that further or the video below to understand pain better.
For some, dry needling is a valuable tool to help people navigate through nociception, central sensitivity, blurred sensorimotor maps, freaked out “protectometers,” or any other great descriptions for that thing we call “pain.” Some people look at you like you have 10 heads when you recommend dry needling. Some are completely convinced it will not help them, while others call themselves “dry needling evangelists.”
For kids, a large part of why I haven’t gone younger than 11 years old is that GENERALLY (not the bold and italics there please) speaking, most kids are healthy and do not have a lot of experience with pain. Generally, pain at this age is highly driven by emotion, fear, and a lot of internalizing of parents’ experiences with pain. Simply put-most kids learn how to cope with pain based on how other family members and their culture breeds them to cope with pain.
Having said all of that—in any person who has very little experience with pain, an injury is often treatable without a lot of passive or manual intervention. I’m not knocking the value of these therapies, but most of these people have not yet learned that “someone else can fix this for me.” They’re open to doing exercises and not afraid of moving. For a few fearful patients, a lot of times we may do manual therapy and/or needling to coax them back into movement. They’ve had pain for so long or on so many instances that they no longer know “which way is up” so to speak. They don’t know what helps or what hurts them, so they just assume avoid all movement and opt for passive treatment.
Needless to say, pain can be very individualized. Even in kids. We have to determine who is the right candidate based on our interpretation of his or her individual pain experience.
What other factors might a PT consider?
Generally, I encourage all patients to start or maintain a level of physical activity. I try and minimize the amount of time that I perform treatments on the patient. The patient is with me maybe 2 hours a week and with themselves (7 X 24)-2 hours. That’s a lot of hours out in the world by themselves. I tell all patients that “movement is medicine.” I’m not expecting my patients to go run a marathon, but everyone has to do something. Kids included. Most kids are pretty active, but some aren’t. I find that age is not a factor here. If a kid is not active, he or she will probably not respond well in the long run to dry needling or to any other interventions. They must learn to take an active approach to caring for themselves.
As for fear of needles: if someone is legitimately terrified of needles-we don’t even go there. This is a screening question I ask all patients when approaching the topic. This can be an issue in kids, though I often find that adults are more afraid of needles than kids. Kids have to get shots all the time for school and have yearly well checks, so they aren’t strangers to needles. Some people just need a little coaching to be ok with needling, while others will tell me the second they find out that we do dry needling that we will NOT be trying this.
Lastly…what caused the trigger point in the first place? Are trigger points really all that bad?
NO! Trigger points happen in everyone. They can be angry little creatures, but they don’t always have to be the problem. Oftentimes they are the result of poor movement strategy. I know several physicians who have learned that dry needling can help patients and refer patients to PT “Just for dry needling.” They are shortchanging the patient when they tell them this. The patient comes in with the understanding that dry needling will fix their problem. What most physicians aren’t trained to do is analyze and retrain movement. And that’s not anything against their exceptional skills. That’s just not a huge part of medical school, residency, and fellowship. That’s part of PT school and advanced PT training.
So, does my kid need dry needling or not?
While there may be exceptions, typically the younger patients (7-13) do not necessarily need dry needling as the first line of defense. Typically, even with the elite young athlete, we do all sorts of kid-friendly and sports-friendly therapy and the kids get better quickly. Sometimes it’s just a matter of quelling their fears and showing them that a little heel or knee pain can get better with some education, strengthening, and proper retraining.’